
It is the question every new L&D manager, HR Manager and Head of Quality eventually asks. It is also the question with no single national answer.
This guide walks through how to think about training hours under the Strengthened Aged Care Quality Standards: where the cadence comes from, what each role typically needs, how the post-November-2025 environment has reshaped the numbers, and where Knowledge Verification can legitimately compress the time without compromising audit evidence.
The truth: there is no single number
Aged care does not have a single legislated figure for annual mandatory training hours. What exists instead is a framework of Outcomes under the Strengthened Aged Care Quality Standards (Aged Care Quality and Safety Commission, 2025) and an expectation that each provider will determine the appropriate training cadence based on:
- The Outcomes that apply to their service
- The roles in their workforce
- The risk profile of those roles
- The currency of the underlying content
The right number, for any given provider, is the number that produces credible workforce capability evidence under audit. Less than that is non-compliant. More than that is wasted seat-time.
The relevant statutory framework is the Aged Care Act 2024, which commenced on 1 November 2025 alongside the Strengthened Quality Standards (Department of Health, Disability and Ageing, 2025a; Aged Care Quality and Safety Commission, 2025). Standard 2 (The Organisation) requires providers to ensure their workforce is competent and skilled for the roles they perform, which is the Outcome most directly tied to training cadence.
A conservative model by role
The Strengthened Aged Care Quality Standards do not prescribe a specific number of training hours per role. What they do prescribe is a set of Outcomes - and each Outcome carries an expectation of auditable workforce capability evidence. The indicative ranges below reflect what a diligent provider would need to assign to meet those evidence requirements across the mandatory topic areas under the Standards (Aged Care Quality and Safety Commission, 2025). They are informed by the scope of the Standards, the risk profile of each role, and the mandatory topic areas the Standards activate for that role.
The third column shows what is achievable for experienced staff when Knowledge Verification is applied to eligible refresher topics - typically a 25 to 30 per cent reduction in annual seat time for staff who can demonstrate existing currency. This compression is only available on stable, moderate-risk topics where a module has been completed within the last two years; high-risk clinical topics and frequently-updated regulatory content still require full completion.
| Role | Induction hours | Annual mandatory hours | With Knowledge Verification | Notes |
|---|---|---|---|---|
| Personal Care Worker | 20-40 | 12-18 | 9-13 | Lower induction at re-deployment from another aged care provider with RPL |
| Enrolled Nurse | 30-45 | 16-24 | 12-18 | Includes clinical scope-of-practice refreshers |
| Registered Nurse | 35-50 | 20-28 | 15-21 | Higher cadence for clinical governance, deterioration, medication |
| Lifestyle / Recreation | 15-25 | 8-12 | 6-9 | Inclusion, dignity, person-centred care emphasis |
| Hospitality / Food Services | 12-20 | 6-10 | 4-7 | Food safety, allergens, dignity of dining |
| Allied Health | 20-30 | 10-16 | 7-12 | Scope of practice plus Standards-aligned modules |
| Clinical Manager / Director of Nursing | 30-45 | 20-30 | 15-22 | Includes governance, leadership, continuous improvement |
| Volunteer | 4-12 | 2-6 | 2-4 | Refresher on dignity, escalation, basic safety |
The Strengthened Standards multiplier
For many providers, mandatory training hours have grown materially since 1 November 2025 (Aged Care Quality and Safety Commission, 2025). The Standards have not added entirely new topics so much as added evidence expectations to existing topics and shifted the audit conversation from completion to application. Each standard now includes specific and auditable actions, making it easier to assess quality and identify areas for improvement (Department of Health, Disability and Ageing, 2025a).
The effect is a multiplier that varies by provider. Across the Ausmed customer base, some providers have seen training hours grow by around 30 per cent. Others have seen them roughly triple. The shape of the multiplier is consistent: more topics now require knowledge-and-evidence pairs (training plus competency observation, or training plus scenario participation, or training plus supervisor sign-off), where previously a completion record alone sufficed.
The operational consequence: providers who do not actively manage cadence will see training hours grow indefinitely. Providers who do actively manage cadence (compressing through KV, focusing scenarios on the highest-risk Outcomes, eliminating orphaned modules) can absorb the Strengthened Standards without increasing total hours.
How to set the right cadence
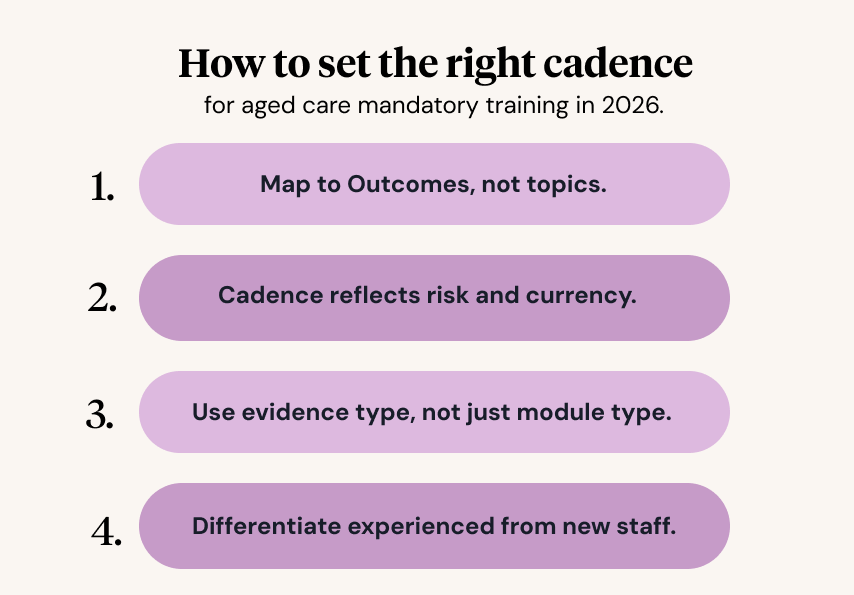
Four principles guide cadence-setting under the Strengthened Standards.
1. Map to Outcomes, not topics. A training matrix that lists topics (manual handling, infection control, medication safety) is harder to audit than one that lists Outcomes. Map each training requirement to the Outcome it satisfies.
2. Cadence reflects risk and currency. High-risk and frequently-updated topics (restrictive practices, medication management, deterioration) need annual cadence. Lower-risk, stable topics (workplace orientation, dignity-of-risk awareness) can be triennial with annual reminders.
3. Use evidence type, not just module type. Some Outcomes are satisfied by a module plus completion. Others require a module plus scenario participation plus supervisor sign-off. The cadence should reflect the evidence requirement, not just the module length.
4. Differentiate experienced from new staff. A worker with five years of experience and a portable learning record should not be required to complete the same induction as a graduate. Recognition of prior learning and Knowledge Verification address this directly.
Where Knowledge Verification compresses hours
Knowledge Verification (KV) is a structured pre-assessment that lets experienced staff demonstrate existing knowledge rather than repeat a module. Done well, Ausmed customer data suggests KV compresses refresher seat time by 40 per cent or more for experienced staff, without compromising audit evidence (Ausmed, 2025).
KV is most useful in three scenarios:
- Annual refresher modules for experienced staff who have completed the full module within the last two years
- Topics where the underlying content is stable and the risk profile is moderate
- Cohorts where most staff are experienced (e.g. tenured personal care workers in a residential site)
KV is not appropriate for:
- High-clinical-risk topics (medication safety, basic life support)
- Topics with significant psychomotor skill (manual handling)
- Frequently-updated regulatory topics (mandatory reporting requirements)
- Onboarding for new starters who have not previously completed the content
Used inside those guardrails, KV can reduce the annual mandatory training burden by 20 to 30 per cent without losing compliance coverage. The savings are reinvested into competency, leadership development, or simply into more time on the floor with residents.
The audit reality
In 2026, the Aged Care Quality and Safety Commission cares about evidence of application, not certificate count (Aged Care Quality and Safety Commission, 2025). An auditor reviewing your training records will not ask whether your PCAs completed 14 hours of mandatory training in the last year. They will ask whether the PCA caring for a specific resident can demonstrate the knowledge required to manage a specific scenario.
Underscoring the seriousness of this shift, the Commission is taking active regulatory action where care obligations are not being met. As of late 2024, only 45 per cent of providers were meeting both Care Minutes and RN targets, and the Commission has put Enforceable Undertakings in place with 11 providers operating 27 individual residential aged care homes (Aged Care Quality and Safety Commission, 2024).
A self-check
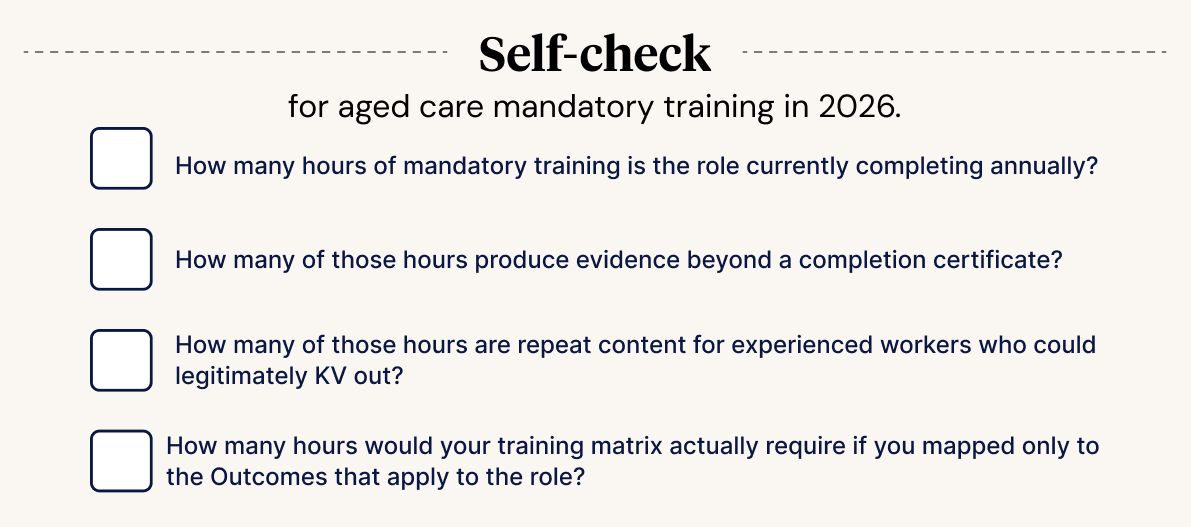
For each role in your workforce, answer four questions:
- How many hours of mandatory training is the role currently completing annually?
- How many of those hours produce evidence beyond a completion certificate?
- How many of those hours are repeat content for experienced workers who could legitimately KV out?
- How many hours would your training matrix actually require if you mapped only to the Outcomes that apply to the role?
The gap between question 1 and question 4 is your over-training. The gap between question 1 and question 2 is your evidence weakness. Most providers carry both gaps simultaneously.
References
Aged Care Quality and Safety Commission (2024) Commission cracks down on aged care providers failing to meet care minutes. Available at: ACQSC media release (Accessed: 26 May 2026).
Aged Care Quality and Safety Commission (2025) Strengthened Aged Care Quality Standards. Available at: ACQSC Strengthened Standards (Accessed: 26 May 2026).
Ausmed (2025) Knowledge Verification: Compressing refresher training for experienced aged care workers. Available at: Ausmed Knowledge Verification (Accessed: 26 May 2026).
Department of Health, Disability and Ageing (2025a) About the new rights-based Aged Care Act. Available at: DoHDA new Act overview (Accessed: 26 May 2026).

