 New
New Clinical Management of Acute Coronary Syndromes
CPDTime.
13m
Published: 14 February 2024


Published: 14 February 2024
Did you know that over 30% of deaths in the Western world can be attributed to acute coronary syndromes (Nickson 2021)?
Furthermore, in Australia, over 200 people are admitted to hospital every day for acute coronary syndrome (ACSQHC 2019).
Acute coronary syndrome (ACS) is an umbrella term used to describe any situation where the blood supply to the heart is suddenly obstructed (AHA 2022).
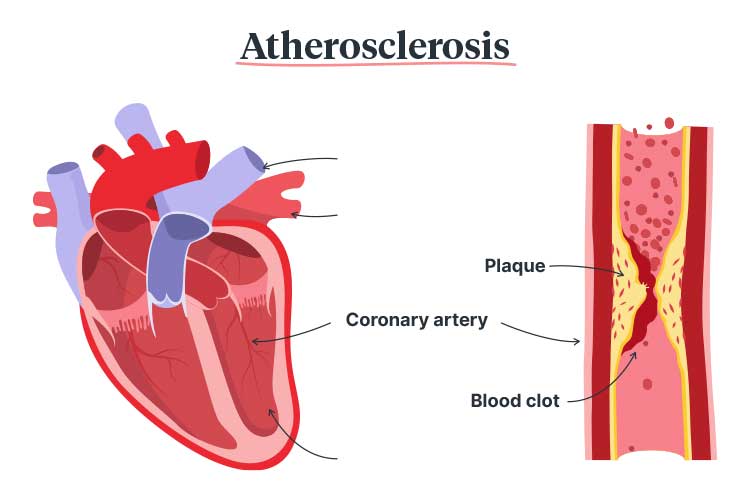
In most cases, the blockage is caused by a thrombosis that decreases blood supply to part of the heart muscle (ACSQHC 2019).
The primary cause of an ACS is atherosclerosis (also known as coronary heart disease), a condition where plaque (made up of cholesterol and fatty materials) builds up and thickens the artery walls (ACSQHC 2019; Shahjehan & Bhutta 2023).
In some cases, an ACS is caused by the spasming and narrowing of the arteries, which impedes blood supply, or spontaneous coronary artery dissection, which occurs when the coronary artery wall tears (Heart Foundation 2023).
If not treated properly, an ACS can be life-threatening (ACSQHC 2019).
Acute coronary syndromes include:
(ACSQHC 2019; Nickson 2021)
Unstable angina describes chest pain caused by an obstructed blood supply to the heart. This may progress into an acute myocardial infarction, which occurs when the blockage injures or causes the death of the heart muscle (ACSQHC 2019).
Certain patients are less likely to receive appropriate interventions (especially invasive management) for an ACS, even if they have been recommended. These include:
(ACSQHC 2019; Worrall-Carter et al. 2016; Walsh & Kangaharan 2017; Chew et al. 2013)
These are some of the issues that informed the development of the Acute Coronary Syndromes Clinical Care Standard.
(Nickson 2021; AHA 2022)

The most common symptom is chest pain or discomfort, which may feel like pressure, tightness, burning or aching (Mayo Clinic 2023). Other possible symptoms include:
(Mayo Clinic 2023)
Note that the symptoms of an ACS often have a sudden onset (Mayo Clinic 2023).
Non-ACS conditions that may cause acute chest pain include:
(Chew et al. 2016)
Even if 12-lead ECG does not indicate STEMI, other life-threatening conditions such as aortic dissection, pulmonary embolism and tension pneumothorax should be considered (Chew et al. 2016).
In 2019, the Australia Commission on Safety and Quality in Health Care released the Acute Coronary Syndromes Clinical Care Standard. This standard aims to ensure all patients presenting with an ACS receive consistent and appropriate treatment (ACSQHC 2019).
The standard contains six quality statements that aim to guide the care of patients experiencing an ACS:
Read: Chest Pain Assessment: What to Do When Your Patient Has Chest Pain
Patients who present with acute chest pain or other symptoms indicative of ACS are assessed using a documented chest pain assessment pathway. Patients should be appropriately informed and provide informed consent for treatment.
(ACSQHC 2019)
Read: 12-lead ECG in the Field
Patients who present with acute chest pain or other symptoms indicative of an ACS should undergo a 12-lead ECG and have the results interpreted within 10 minutes of first emergency clinical contact. The ECG must be performed by an appropriately experienced clinician.
This is to ensure that ACSs are identified as soon as possible and treatment can be commenced.
(ACSQHC 2019)
Patients experiencing a STEMI should undergo percutaneous coronary intervention (PCI) or fibrinolysis if emergency reperfusion is deemed clinically appropriate (ACSQHC 2019).
Based on the current Heart Foundation guidelines:
(Chew et al. 2016)
Patients experiencing an NSTEACS should be managed depending on their anticipated risk of severe cardiac issues in the future.
In order to evaluate this risk, the clinician may use risk assessment tools such as:
Any treatments should be planned using a shared decision-making process, and patients’ preferences should be taken into account.
(ACSQHC 2019)

Coronary angiography is a procedure in which dye is released into the patient’s arteries. Through an x-ray, this dye is able to indicate the location and extent of arterial blockages.
It is recommended that patients experiencing an NSTEACS consider undergoing coronary angiography if the anticipated risk of severe cardiac issues in the future is medium or high.
(ACSQHC 2019)
Prior to discharge, patients who have experienced an ACS should work with clinicians to develop an individualised care plan containing:
Within 48 hours of discharge, a copy of this plan should be forwarded to the patient and their general practitioner or ongoing clinical provider.
(ACSQHC 2019)
Secondary prevention strategies such as lifestyle changes, medicines and rehabilitation are essential in reducing the risk of future adverse events (Chew et al. 2016).
Question 1 of 3
If emergency reperfusion can not be performed within 90 minutes, what treatment should the patient generally receive?


Ausmed Education is a Trusted Information Partner of Healthdirect Australia. Verify here.