 New
New 5-Lead ECG Placement and Cardiac Monitoring
CPDTime.
4m
Published: 27 April 2023


Published: 27 April 2023
In order to accurately and correctly assess a patient using 5-lead monitoring, it is necessary to understand how ECG works, know how to prepare the patient and be able to follow the standardised system for electrodes and their placements.
An electrocardiogram (ECG) is a non-invasive method of monitoring the electrophysiology of the heart (Mayo Clinic 2022).
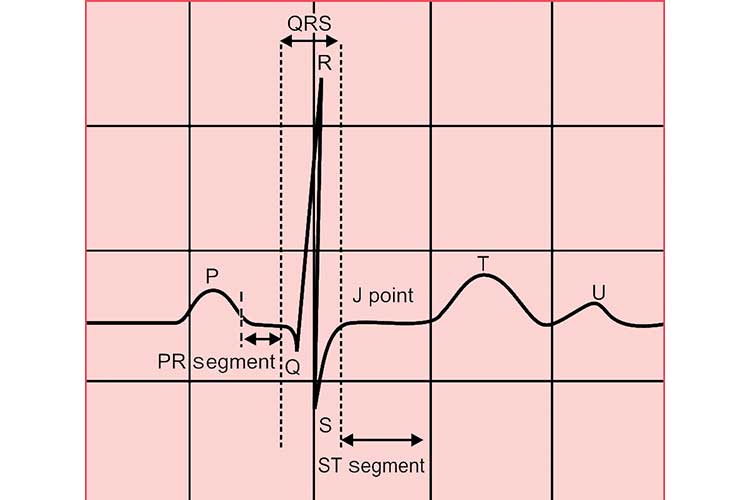
An ECG machine records changes in electrical activity by drawing on moving paper known as an electrocardiograph. The paper moves at a speed of 25 mm per second, and the ECG machine plots time on the x-axis and voltage on the y-axis. On the electrocardiograph, one second is represented by five large squares. These large squares are broken into five smaller squares representing 0.04 seconds each. When the ECG machine is plotting the patient’s electrical activity, an increase of one mVolt in voltage moves the stylus by 1 cm (Sattar & Chhabra 2023).
While ECG is commonly used across a variety of medical settings, it plays a particularly important role in the haemodynamic assessment of intensive care unit (ICU) patients (Khan 2020).
All ICU patients generally require continuous ECG monitoring if clinically unstable. Continuous ECG monitoring can improve the detection of clinical deterioration (Khan 2020; Moss et al. 2017).
An ECG involves the placement of electrodes onto the patient’s torso and/or limbs. The electrodes are connected to an electrocardiograph, which displays a pictorial representation of the patient’s cardiac activity (Better Health Channel 2023).
The waves detected and visually displayed through ECG illustrate the sequence of depolarisation (positive current) and repolarisation (negative current) generated by action potentials (electrical impulses) of the atria and ventricles in the heart (Klabunde 2022a).
In ICU settings, ECG is generally used for continuous monitoring of the patient’s heart rate and the detection of any potentially fatal cardiac abnormalities such as arrhythmias, but may also serve a diagnostic purpose (Gandhi & Lewis 2016).

ECG measures the electrical activity of the heart from several leads (viewpoints) in order to construct a picture of the patient's cardiac function using voltage on the vertical axis against time on the horizontal axis (Cables and Sensors 2016).
Each lead has its own code name and represents the voltage difference between two electrodes. There are two types of leads:
| Lead type | Leads included | How they work |
|---|---|---|
| Bipolar leads (i.e. standard limb leads) | I, II, III | Measure the voltage difference between one positive electrode and one negative electrode. |
| Unipolar leads (i.e. augmented leads and chest leads) |
|
Have a single positive electrode and use a combination of the other electrodes as a composite negative electrode. |
(Cables and Sensors 2016; Klabunde 2022b)
Commonly used lead systems include:
(Cadogan 2022)
12-lead monitoring is generally considered the standard form of ECG and provides the most information, however, it is not always feasible. Limb movement, tremor, anxiety and cold extremities may interfere with ECG readings, causing them to be poor quality and consequently more difficult to interpret (Khan 2015).
As a result, torso leads are preferable as they allow for better quality ECGs. 3 and 5-lead monitoring take electrodes that are used for the limbs in 12-lead monitoring and instead place them on the chest wall in order to reduce artifacts (ECG signals that are from sources other than the heart) caused by patient movement (Khan 2015; Sampson 2018; Philips 2019).
5-lead monitoring is the same as three-lead monitoring, but with two additional electrodes that enable the monitoring of extra leads and help improve ST elevation readings (Cables and Sensors 2016). It is able to monitor the leads I, II, III, aVR, aVL, aVF and V (Phillips 2019).
Correct placement of electrodes is crucial.
The placement of electrodes for ECG monitoring is standardised to ensure that the information gathered is accurate and can be compared with records from other occasions. To ensure accurate results, the patient must also be correctly prepared both physically and psychologically (ADInstruments 2019).
Poor electrode placement can result in mistaken interpretation, and then possible misdiagnosis, patient mismanagement and inappropriate procedures (Khunti 2013).
ECG electrodes are colour-coded, and each is identified by a specific code that refers to its intended placement. There are two coding systems currently in use:
Both systems are described in the table below.
| Location | Code (AHA) | Colour (AHA) | Code (IEC) | Colour (IEC) |
|---|---|---|---|---|
| Right arm (inner wrist) | RA | White | R | Red |
| Right leg (inner ankle) | RL | Green | N | Black |
| Left arm (inner wrist) | LA | Black | L | Yellow |
| Left leg (inner ankle) | LL | Red | F | Green |
| Chest | V | Brown | C | White |
(ADInstruments 2019; Cables and Sensors 2016; PanSW 2013)
Note: The following guide uses the AHA system.
| RA placement | WHITE directly below the clavicle and near the right shoulder. |
| LA placement | BLACK directly below the clavicle and near the left shoulder. |
| RL placement | GREEN on the right lower abdomen. |
| LL placement | RED on the left lower abdomen. |
| V placement | BROWN on the chest - the position depends on your required lead selection (4th intercostal space, the right side of the sternum). |
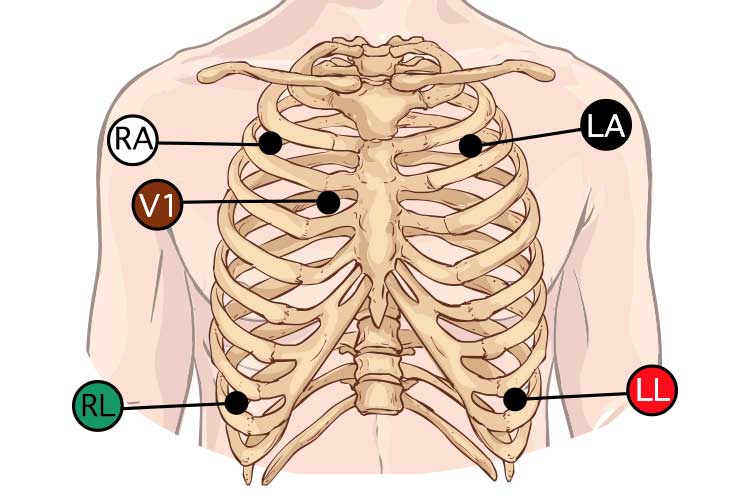
(Elsevier 2022; Pope 2002)
While 5-lead monitoring can provide an adequate amount of information, if something of concern is noted, such as a cardiac arrhythmia, 12-lead monitoring may be implemented in order to garner a better idea of the issue (Kleber 2019). Other investigations such as echocardiograms and blood tests may need to be considered.
Arrhythmias may cause haemodynamic instability, which can lead to loss of consciousness (UHealth 2018). You should notify any rhythm abnormalities to the medical team and compare the patient with their previous 12-lead ECG (if one has been conducted).
Remember to always perform lead placement at the commencement of your shift as well as before and after repositioning the patient to ensure all electrodes and cables are in the correct position.
Question 1 of 3
True or false: 5-lead monitoring involves placing limb electrodes on the torso.


Ausmed Education is a Trusted Information Partner of Healthdirect Australia. Verify here.